Femoral Popliteal & Femoral Distal Bypass
All emboli of the lower extremity, including a proximal saddle embolus at the aortic bifurcation, can be removed through the common femoral artery using Fogarthy catheters. By passing these through the embolus, and by inflating the small balloon, the clot can be withdrawn and the flow restored. An alternative to embolectomy is thrombolytic therapy. A percutaneous catheter directs thrombolytic agents, such as streptokinase or tissue plasminogen activator, directly into the clot to dissolve it.
Preoperative Preparation
- Systemic heparinization prevents extension of thrombosis & dissemination of further emboli from their source.
- Treatment of heart failure or dysrhthmias may be required.
- Both groins & legs are prepared & draped. The feet may be placed in sterile transparent bags to check for restoration of circulation.
Incision
Vertical, at the mid-inguinal point, from a few centimetres above the inguinal ligament & extending distally over the course of femoral artery.
Procedure
- Deepen the incision through the subcutan fat & divide the femoral sheath to expose the common femoral artery & its superficial femoral & produnda branches.
- The femoral vein, lying medially, must be protected.
- Pass a rubber sling around the artery & gently lift it forwards & pass the slings around the branches also.
- After giving a bolus dose of heparin intravenously, apply angled vascular clamps to the three main vessels.
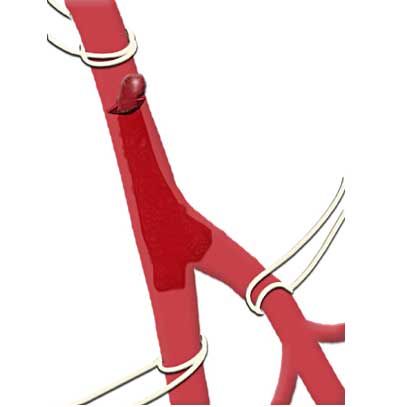
- Make a small transverse arteriotomy over the common femoral artery near the origin of its profunda femoris branch.
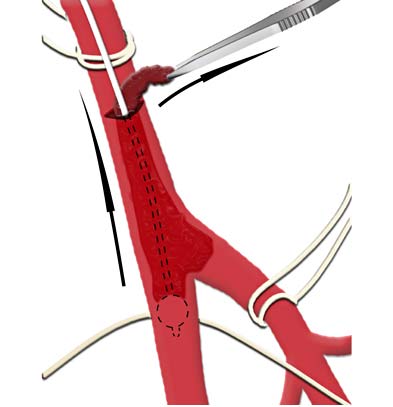
- To check the in-flow, gently release the clamp on common femoral. If the in-flow is poor a Forgarty (size 5F) should be passed proximally to retrieve clot & restore the inflow. The clamp is reapplied.
- Release the clamp on the superficial femoral artery to assess the back flow. A Fogarty catheter (size 4F) is passed to remove any distal embolus.
- Repeated passage of this catheter may be required until no further clot is seen.
- This is followed by infusion of heparinized saline. The same procedure is repeated for profunda femoris artery.
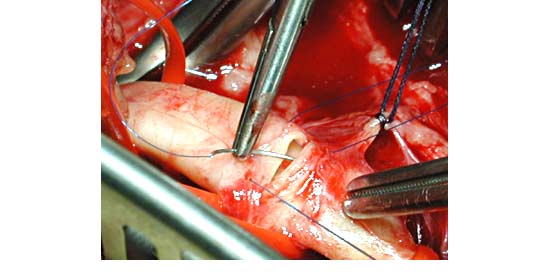
- Once the distal circulation is restored, the arteriotomy can be closed.
- The distal circulation will be confirmed by the return of pulses and its completeness by Doppler & occasionally angiography.
Intra-operative Problem
Occastionally it is difficult, preoperatively, to differentiate between embolus & a superimposed thrombosis on an already diseased artery. This can be resolved by a per-operative angiogram & may require a bypass.
Closure
Routine, in layers
Postoperative Management
Will include long-term anti-coagulation to prevent recurrent embolization.