Cardiac Valve Surgery
Preoperative Preparation
- The timing & the type of valvular replacement is ascertained by clinical, echocardiographic & cardiac catheterization data.
- Replacement of an aortic or mitral (rarely tricuspid), both for stenotic & regurgitant lesions requires cardiopulmonary bypass.
- Valve repair rather than replacement is employed where possible.
- Prosthetic valves may be mechanical (longer lasting but require long-term anticoagulants) or tissue (prone to short-term failure). We describe here the placement of a mechanical valve.
Incision
Median sternotomy
Procedure
- Divide the pericardium vertically starting from the ascendingaorta superiorly to the diaphragm inferiorly.
- Establish cardiopulmonary bypass as described in Coronary Artery Bypass surgery.
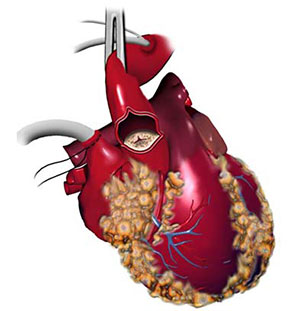
- Expose the aortic valve by an aortotomy over the anterior wall of the aorta.
- The mitral valve can be exposed by an incision over the posterior wall of left atrium parallel to the inter-atrial groove.
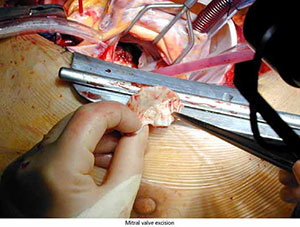
- Excise the diseased valve ensuring no debris falls into the ventricular cavity.
- Preservation of part of the posterior leaflet of mitral valve reduces the risk of ventricular disruption.
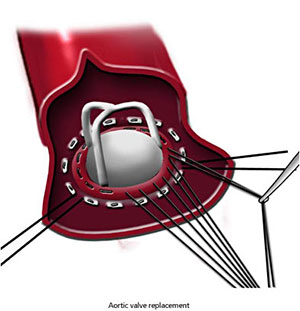
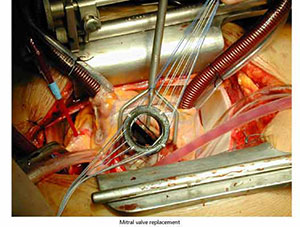
- The annulus of the new valve is sutured to the native annulus by the parachute suturing technique.
- Remove all debris & air before closure of the aortotomy or atriotomy.
Intra-operative Problems
If the annulus is friable, sutures can cut out resulting in paravalvular leak. This can be buttressed by teflon pledgets.
Closure and Drainage
The sternum should be closed by interrupted steel wire sutures. Pericardial drains are used for free drainage.
Main Postoperative Complications
Include complications of bypass, cerebrovascular accidents (2-5%), paravalve leaks & thromboembolic & bleeding complications. Also, valve failure & endocardititis.