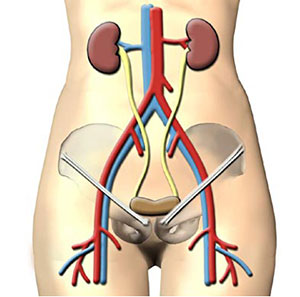
Aorto Bifemoral Bypass
This operation for aorto-iliac occlusive disease is less frequently performed since the advent of effective percutaneous balloon angioplasty with or without stent placement.
Incisions
Full length midline to expose the abdominal aorta & vertical groin to expose the common femoral arteries on each side.
Procedure
- After a full laparotomy, expose the aorta from below the left renal vein as in a aneurysm repair.
- Divide the peritoneum over the aorta continuing down to expose both common iliac arteries.
- Palpate the aorta & the iliac arteries to determine the extent of the disease & select the site of proximal anastomosis, avoiding large calcified plaques. The aortic segment between left renal vein & the inferior mesentesic artery is best.
- If there is total aortic & occlusion, transect it & construct an end-to-end anastomosis with the proximal graft. Otherwise, an end to side onlay anastomosis is preferable to preserve perfusion of the internal iliac arteries.
- After systemic heparinization, aortic control is achieved with vascular clamps.
- A pulsatile inferior mesenteric artery with wide ostia should be preserved.
- Select a bifurcated dacron graft of appropriate size & trim the excess of the body of the graft leaving only few centimeters to avoid kinking of its limbs.
- Construct the proximal anastomosis using synthetic non-absorbable sutures.
- On completion of the aortic anastomosis, apply clamps to each limb of the graft & release the aortic clamp to test its integrity.
- Expose the common femoral artery below the inguinal ligament & place separate rubber slings around common femoral, superficial femoral & profunda femoral arteries.
- Make tunnels retroperitoneally & under the inguinal ligaments, through which to pass the limbs of the graft to the groin incisions. It is preferable to make these tunnels prior to heparinisation.
- Apply clamps to the common, superficial & profunda femoral arteries & make a longitudinal arteriotomy above the bifurcation. The distal anastomoses of graft to femoral arteries are completed in an end to side fashion. Each limb is flushed before completing the anastomosis.
- After completion clamps are released sequentially to avoid declamping shock.
- Finally, the circulation to both feet is checked.
Intraoperative Problems
Aortic clamps can cause fracture of calcified plaques & tear the wall of aorta. This can be controlled by higher application of the aortic clamp & buttress suturing using dacron pledgets.
Main Postoperative Complications
Are similar to those occurring after aortic aneurysm repair.