Amputations for Ischaemia
Amputations for Ischaemia (Above & below knee)
Preoperative preparation
- The level of amputation is influenced by viability of the soft tissues & functional requirements of the patient. Therefore, informed consent is taken for a more proximal level then you would intend.
- Give prophylactic antibiotics
Anaesthesia
General or spinal.
Procedure
- Prepare the skin & apply the drapes to seal off the infected or necrotic part of the limb.
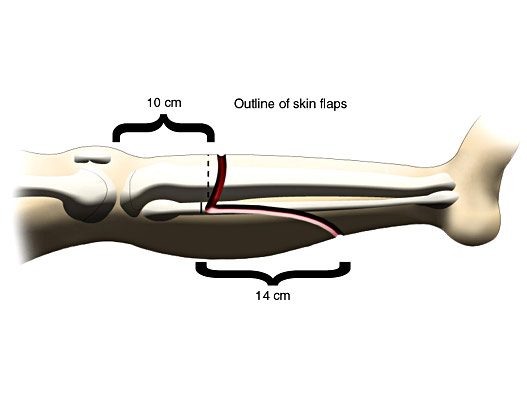
- Mark the proposed skin flaps with a sterile skin marker.
- For above knee amputations, anterior & posterior myoplastic flaps should be roughly the same lengths with their base at the level of bone section.
- For below knee, a long posterior myoplastic flap is configured to construct the stump.
- Remove all dead muscles leaving behind bleeding, red & contracting edges.
- Ligate & divide major vessels at lower levels & main nerves at higher positions.
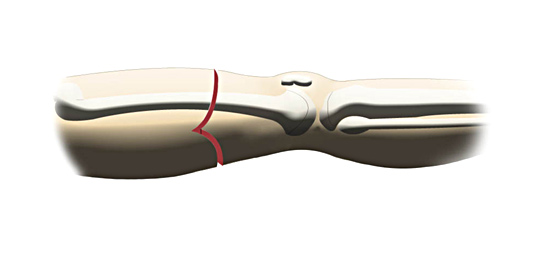
- Divide the periosteum & cut the bone with a Gigli or power saw. The fibula is transected higher than the tibia in a below knee amputation.
- The bone ends are rounded & may be sealed with bone wax.
Closure and Drainage
- Suture the flaps together without tension starting with muscle.
- Handle the skin carefully & close with staples or interrupted nylon sutures.
- Insert a suction drain.
- Apply a pressure dressing over the stump.
Postoperative Management
Multi disciplinary care involving nurses, physiotherapists, occupational therapists, prosthetists & social workers brings the best rehabilitation for these patients. Main post operative complications Include flap necrosis, infection & dehiscence of stump. Later on, phantom limb sensation & pain.