Abdominal Aortic Aneurysm Repair
Repair may be necessary as an elective procedure for which a full pre-operative work-up & preparation can be planned. The luxury is not available in the emergency situation. Here we describe the repair of an infra-renal aortic aneurysm, the usual site. The principles are similar for the emergency & elective situations. Extension of an aneurysm above this level requires more complex control & reconstruction.
Incision
Long midline from the xyphisternum to the symphysis pubis.
Procedure
- After a full laparotomy, displace the omentum & large bowel superiorly & place the small bowel with its mesentery into a plastic bag.
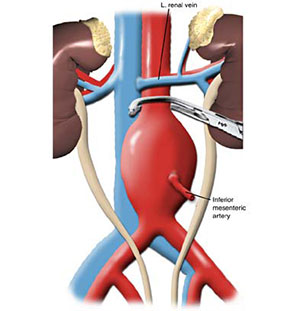
- Divide the peritoneum at the ligament of Treitz. Mobilise the duodenum & expose the neck of the aortic aneurysm & renal vein, which crosses it.
- The renal vein is retracted upwards to gain additional space for the application of aortic clamp above the aneurysm.
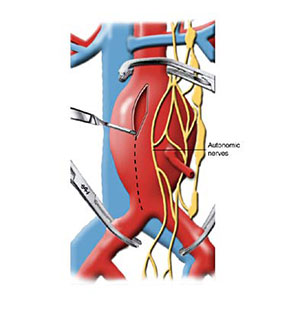
- Continue the incision of the peritoneum longitudinally over the anterior surface of the aorta passing to the right of inferior mesenteric artery & across the bifurcation.
- Identify & protect the ureters on each side as they cross the iliac vessels.
- The common iliac arteries are exposed on the anterior, lateral & medial aspect in preparation for clamp placement. Great care is needed to avoid injury to iliac veins which cross underneath.
- Systemic vascular clamps are then applied to the distal common iliac arteries.
- After clamping above & below, open the aneurysm through a linear arteriotomy to the distal extent of aneurysm.
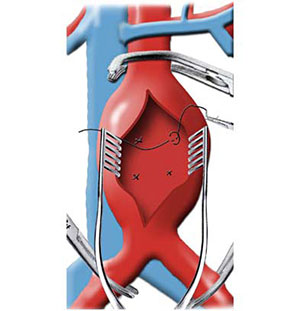
- Remove the mural thrombus from inside the lumen & control the back bleeding from lumbar arteries.
- Prepare the aortic cuff ↦ openings of the iliac arteries. If the aneurysm is not involving iliac arteries then it is preferable to place a straight aortic prosthetic graft. Iliac extension will necessitate a trouser graft attached distally.
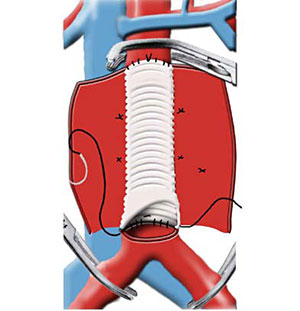
- A pre-clotted knitted Dacron graft of appropriate size is stretched & tailored to fit the aortic defect.
- Suture the proximal end of the graft with a continuous non-absorbable suture &, when complete, apply a vascular clamp distally & release the aortic clamp slowly to check the integrity of the anastomosis.
- Cut the dital graft to the correct size.
- Next, construct an anastomosis over the ostea of both iliac arteries with a running suture.
- Just before the completion of the anastomosis, the aortic clamp is opened momentarily to dlush out any clots & debris that may have accumulated in the aorta or graft.
- Each lef should be opened sequentially after prior warning to the anaesthetist.
- Close the aneurysm sac and peritoneum over the graft.
- Check the circulation in both legs as an embolectomy may be required.
- Before closure, check the adequacy of blood supply to the sigmoid colon.
Main Postoperative complicaitons
Include anastomotic leakage, graft occlusion, distal emboli, renal faulire & paralytic ileus. Later, graft infection & aorto-enteric fistula may occur.
Endovascular Repair
A selected group of patient with abdominal aortic aneurysms can be managed with endoluminal grafts which entails insertion of a folded endoprosthesis via the femoral artery under image guidance. This technique is currently under evaluation.