Lumbar Disc Surgery
Pre-operative Preparation
The indications for surgery must be satisfied. CR, MRI or myelography must confirm the presence of the prolapsed disc, and the level.
Anaesthesia
General
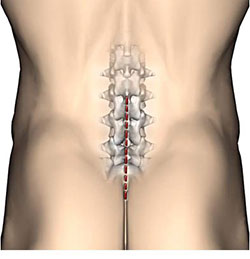
Position
The patient lies prone with pillows under the chest and hips. The spine is flexed by breaking the table.
Incision
Midline over the lumbar spine.
Procedure
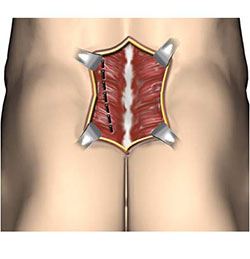
- The fibromuscular attachments on the appropriate side are detached from the spinous processes.
- Next, use an osteotome to scrape the muscles and periosteum from the spinous processes and laminae and inser self-retaining retractors.
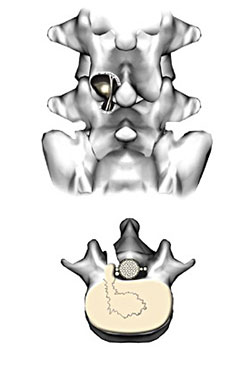
- Access to the spinal canal is gained by excising a space through the ligamentum flavum which bridges the interlaminar space. The contiguous laminae are nibbled away, with an angled bone punch, to create a window to display the nerve root.
- Gently retract the dura and nerve root medially with a dural retractor.
- The protruding disc comes into view.
- Make a cruciate incision in the annulus fibrosis covering the disc and, with pituitary rongeurs, extract the nucleus pulposus either intact or in fragments. Remove all detachable tissue.
- Control all bleeding, especially from epidural veins.
Closure
The lumbodorsal fascia and skin, in layers.
Postoperative Management
Nurse flat for twelve hours post-op. Then mobilise, with gradual introduction of flexion and extension exercises.
Main Postoperative Complications
Include urinary retention and disc space infection, which is serious but rare. Persistent pain may be due to a number of causes and might require re-operation.
Miscrodiscectomy
Is similar to the above operation but the exposure is much smaller and the procedure is carried out with an operating microscope. Accurate diagnosis of the level of the disc is necessary and bleeding can be difficult to control but morbidity and length of hospital stay are less.
Laminectomy
Involves removal of the spinous processes and laminae on either side, over a number of levels, usually for spinal decompression for spinal stenosis or the removal of extra or intradural masses.