Hip Procedures
Approaches to the hip
Anterior, for open reduction of a CDH, tumour surgery, acetabular fracture fixation, arthrodesis or biopsy. Anterolateral. For reduction of a femoral neck fracture, synovial biopsy or hemiarthroplasty. Lateral, Direct or transtrochanteric. For total hip arthroplasty, hemiarthroplasty or reduction of an anterior dioslocation.
Posterior. For total hip arthroplasty and fixation of pelvic or posterior acetabular fractures.
We describe here, briefly, the anterior and posterior approaches but further details of these and the other approaches, their advantages and disadvantage, can be obtained in fuller orthopaedic texts.
Anaesthesia
General or spinal
Position
Anterior. Supine with a sandbag under the affected buttock.
Posterior. Lateral decubitus.
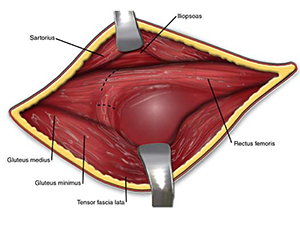
Anterior
Incision
From the mid-point of the iliac crest to the anterior superior iliac spine, then distally for 10cms.
Procedure
- Develop the interval between sartorius and tensor fascia lata (TFL.) Take care of the lateral cutaneous nerve of the thigh which is retracted medially.
- Free attachment of gluteus medius and tensor fascia lata off the ilium.
- Reflect sartorius medially and TFL laterally to expose gluteus medius and rectus femoris.
- Ligate the ascending branch of the lateral circumflex femoral artery.
- Detach both origins of rectus femoris and expose the joint capsule.
- After capsulotomy, dislocate the hip by external rotation.
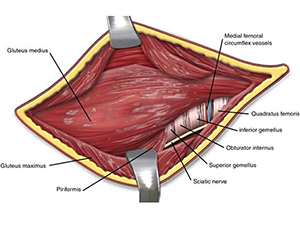
Posterior
Incision
From the posterior aspect of the greater trocanter towards the posterior superior iliac spine (10cms) and distally down the postero-lateral aspect of the thigh.
Procedure
- Incise the fascia lata and plit the gluteus maximus.
- Separate the two parts of gluteus minimus exposing the sciatic nerve.
- Internally rotate the hip and transfix and divide the combined tendons of obturator internus and the gamelli close to the bone and reflect them posteriorly to protect the sciatic nerve.
- Divide the proximal quadratus femoris to expose the posterior joint capsule.
- Divide the capsule and dislocate the joint by flexion, adduction and internal rotation.