Tendon repair
Tendon injuries occur most frequenctly in the hand. Tendons, when cut or torn, become frayed and longitudinal sutures tend to cut out. When contained in a synovial sheath, considerable retraction may occur. Less retraction and better healing will occur where they are surrounded by paratenon. Tendon repair should not be regarded as a minor procedure. Particular specialist care should be provided in the difficult zone, where the flexor tendons lie within the fibrous flexor sheath, from the distal half of the hand to the distal third of the middle phalanx. Fractures should be stabilised before tendon repair. Secondary tendon repairs may be performed but it is important that the anastomosis occurs in healthy tissues or, if the bed is scarred, a tendon graft should bypass it.
Anaesthesia: General or regional and a pneumatic tourniquet is essential.
Incision
There is often a laceration in place as the cause of the tendon damage. It is usually necessary to extend the access by incision in both directions parallel to the tendon in order to locate proximal and distal ends.
Procedure
- The divided tendon ends are located and held by fine needle transfixion. It is critical to correctly match the tendon ends when multiple tendons have been divided.
- Trim and freshen the lacerated ends of the tendons.
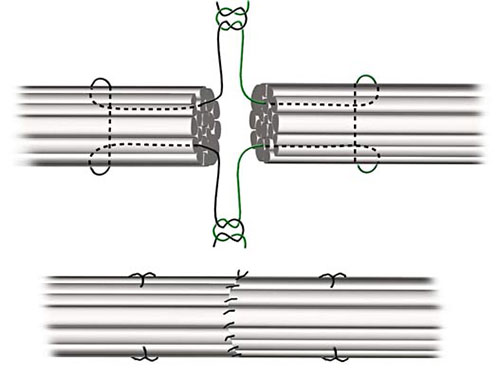
- The tendon ends are anastomosed using a specific technique, such as that described by Kessler with a synthetic monofilament suture on an atraumatic needle.
Closure
Routine skin closure.
Postoperative Management
Protect the suture line from stress with appropriate splintage. Early passive and then active movements, particularly for tendons within tendon sheaths, lessens the tethering affect of adhesions.
Main Postoperative Complications
Include anastomotic breakdown, stiffness, and loss of function.