Carpal Tunnel Release
Pre-Operative Preparation
Median nerve conduction delay at the level of the wrist should be shown on electromyographic studies/
Anaesthesia
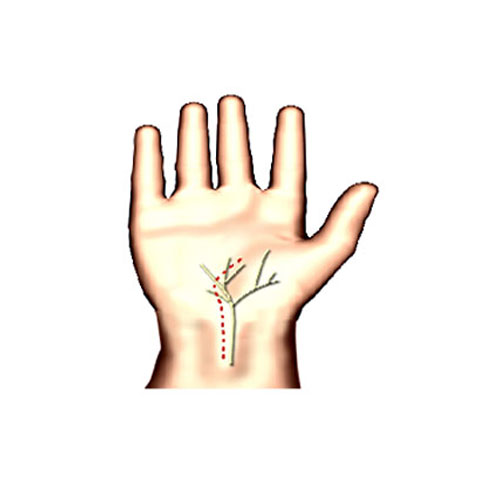
General, local or regional anaesthesia. A tourniquet is applied to obtain a bloodless field and a malleable lead hand may be used to stabilise the hand.Incision: Is curved from the ulnar border or palmaris longus tendon, where it crosses the wrist crease to extend into the midpalm
Procedure
- The incision is deepend until the flexor retinaculum is reached.
- Care is taken not to injure the superficial palmar branch of the median nerve.
- The middle of the fibrous flexor retinaculum is divided longitudinally. Great care is taken not to injure the median nerve which may be protected with a dissector.
- The retinaculum is fully divided to release the nerve and it may also require freeing from adhensions.
Closure
The skin only is closed & the hand is dressed in the position of function.
Postoperative management
Start hand physiotherapy early.
Main Postoperative Complications
Nerve damage or failure to release the median nerve sufficiently.