Laparoscopic Cholecystectomy
Summary Video
Preoperative Preparation
- Assess the risk of bile duct stones (by history, liver function tests & bile duct appearance on US) & plan treatment with an ERCP, if necessary.
- Informed consent includes a warning of the rare but possible risk of bile duct injury.
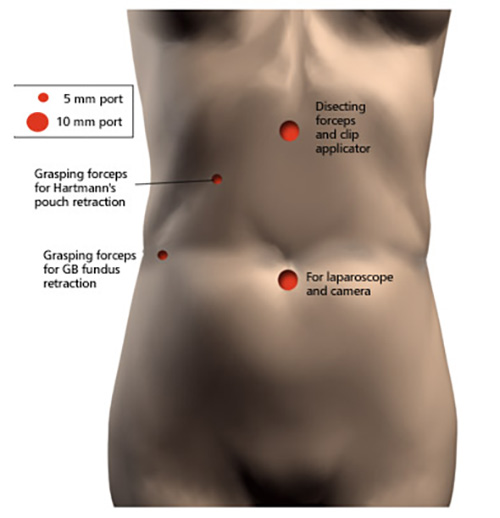
Procedure
- An assistant places a grasping forceps via the lateral 5mm port & pushes the fundus of the gallbladder & liver up towards the right shoulder. This allows the operating surgeon to see & grasp Hartmann's puch & retract it laterally & distally. Divide the peritoneum close to the gallbladder & using gentle dissection, with minimal & judicious use of diathermy, the cystic duct & artery are displayed. As in the open operation, no structures are divided until both the cystic duct & artery are clearly identified being cognisant of potential injury to the CBD.
- Metal clips are applied first to the cystic duct - an operative cholangiogram can be performed beforehand. It is then divided between clips, followed by the cystic artery.
- Next, dissect the gallbladder from the liver with diathermy dissection using a scissors or hook.
- Before detaching the fundus from the liver, ensure haemostasis.
- Irrigate & aspirate saline to lavage the right upper quadrant.
- The gallbladder is then removed via any of the 10mm ports but if any spillage of bile or stones has occurred during the dissection then a bag is used for retrieval.
Main Postoperative Complications
Include injury or division of the CBD. Beware of a diathermy injury in a laparoscopic cholecystectomy.