Anterior Resection of the Rectum
Preoperative Preparation
- Localisation & staging of the tumour with sigmoidoscopy, endo-anal ultrasound & abdominal CT.
- Down-staging with chemo-radiation for locally advanced tumours.
Position
- Lithomy with Trendelenburg
Procedure
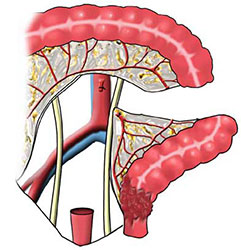
- After a full laparotomy, mobilise the sigmoid colon by dividing its lateral adhesions & peritoneal reflection. Take care to identify & preserve the left ureter & gonadal vessels.
- Mobilisation up to & inlcuding the splenic flexure, as described in 'Left Hemicolectomy', may be required; & it is continued down to the upper rectum.
- The inferior mesenteric vein is ligated prior to tumour mobilisation. The inferior mesenteric artery is divided & ligated close to the aorta, in order to harvest the draining nodes.
- Next, divide the vessels in the mesocolon towards a selected level of descending colon suitable for bringing down as the proximal anastomosis. Divide the bowel at this point with a linear cutting stapler.
- Divide the peritoneum around the rectum & then retract the distal colon forwards in order to develop the plane between the mesorectum & the presacral fascia, distal to the sacral promontory. Identify & preserve the pre-sacral nerves. Stay anterior to the pre-sacral fascia to avoid the sacral veins.
- Low rectal tumours (<12cm from the anal margin) require full mesocrectal excision while those > 12cm are thought not to.
- The rectum with its intact mesorectum (for a low tumour) is mobilised posteriorly as far as the coccyx & the lateral ligaments of the rectum are divided & ligated or diathermised.
- In front of the rectum continue the dissection distally, behind the vagina in the female, & the seminal vesicles in the male.
- The rectum is divided distal to the tumour (> 2cm) using a transverse stapler.
- When hand sewing, a single layer anastomosis is completed using a parachute technique.
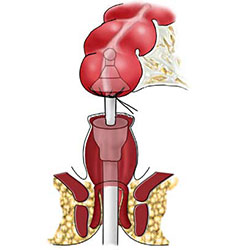
- For a stapled anastomosis, first place a purse-string suture around the proximal stump of descending colon & tie it around the anvil which is detached from its stapling gun.
- Next, an assistant passes the circular stapling device transanally, its inner shaft is opened to penetrate the stapled rectal stump & is joined to the shaft of the anvil.
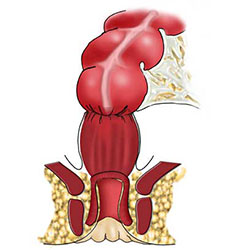
- Approximate the head & anvil of the stapling gun &, when the two ends of bowel are firmly apposed, it is fired. The gun both cuts & staples, forming an air-tight anastomosis.
- The integrity of the completed anastomosis is tested by air insufflation of the rectum.
- If there is concern about the anastomosis or it is low (< 7cm from the anal verge), it is wise to defunction with a temporary loop ileostomy.
Main Postoperative Complications
- Include anastomotic dehiscene & erectile dysfunction in the male. Later on, tumour recurrence may occur.