Vascular Anastomosis
The following techniques may be required for some of the vascular operations in this module and are therefore not repeated with each operation, but should be considered. Any variation from the points listed below will be mentioned under the specific operation.
Pre-operative Preparation
- Get as much information as possible about the relevant vascular anatomy & pathology by appropriate imaging.
- Carefully assess cardiac & pulmonary function & correct abnormalities where possible.
- A nasogastric tube is inserted in abdominal proocedures.
- Place a urinary catheter to monitor the urinary output.
- Use priphylactic antibiotics especially when inserting foreign graft materials.
- Group & cross-match adequate supplies of blood.
- Adequate resuscitation with fluids & blood is important in the emergency situation.
- Obtain informed consent.
Anaesthesia
Cardiac & aorto-iliac operations & prolonged peripheal operations require general anaesthesia. Shorter operatiosn on limb blood vessels may be performed using local, regional or spinal anaesthesia.
Position
Supine in most of the cardiovascular operations described.
Incisions
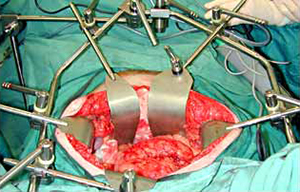
Median sternotomy is the usual approach for heart surgery. Midline abdominal for aorto-iliac operations & exposure is best maintained using a fixed table retraction system (e.g. Omnitract). Transverse abdominal incisions or the retroperitoneal approach are less commonly used. Durectly over the vessel are best in peripheral procedures.
Procedures
Requirements include:
- Atraumatic vascular clamps & dissectors, vascular slings, atraumatic (umbilical) catheters, Fogarty embolectomy catheters & intraluminal shunts.
- Magnifying loupes (x2.5)
- Specialised synthetic non-absorbable sutures.
- Irrigation solution (5000 units of heparin in 500ml saline).
- Synthetic grafts; may include many different materials but are mostly made of either Dacron (knitted, requires pre-clotting, or woven), or expanded polytetrofluoethylene (PTFE)
- A range of guide-wires, endovascular ballons & stents as well as an image-intensifier for endovascular procedures.
- Bypass facilities for open heart surgery
Give 5000 units of heparin intravenously & allow three minutes for it to circulate before applying vascular clamps.
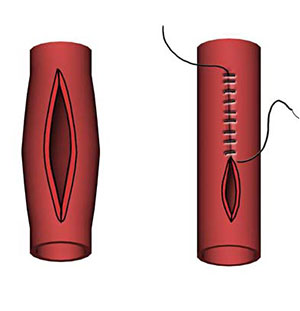
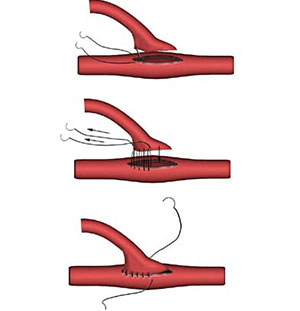
An arterotomy may be best performed longitudinally because:
- It is easier
- It can be extended
- It is easier to close; but does noarrow the vessel more than a tranverse arteriotomy which preferred for embolectomies.
Arterial repair can be simple, with a continuous everting suture.
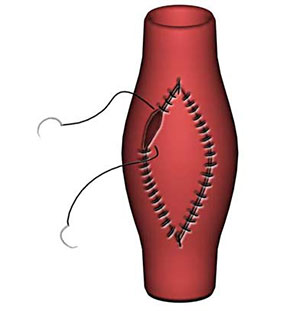
By a patch of autologous vein or synthetic material. This is preferable to simple closure as it reduces risk of vessel narrowing.
>
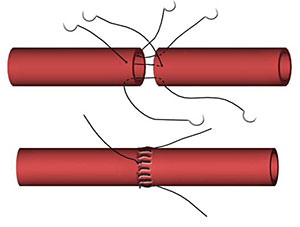
An arterial anastomosis can be end to end, or end to side.
An endarterectomy involves the development of a well-defined plane within the innermost layers of the media in order to dissect off deseased atheromatous intima. It may be performed open (using a blunt MacDonald's or Watson Cheyne dissector) or closed. When a natural end-point is not reached 'tack-down' sutures, a vein patch or some other procedure is required to minimize turbulence at the end point.
Closure and Drainage
Routine closure in layers depending on the anatomic site. In traumatic situations it is important to cover a vascualr anastomosis by primary closure or repair of a defect with plastic techniques, if necessary. Closed suction drains may be used.