Haemorrhoidectomy
Preoperative Preparation
Phosphate enema. Metronidazole at induction.
Anaesthesia
General or spinal
Position
Lithotomy or jack-knife
Procedure
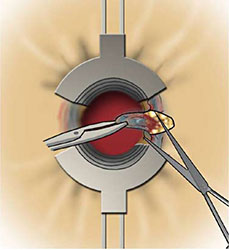
- After procto-sigmoidoscopy, identify the haemorrhoids that need to be excised - usually a left lateral, right posterior & right anterior.
- Expose the left haemorrhoid with an anal retractor, Parks or Eisenhammer.
- Bupivicaine & adrenaline is infiltrated around the haemorrhoid for resection.
- Apply an artery forceps to the gaemorrhoid at the anal margin for restraction.
- Using scissors or diathermy make a v-shaped incision in the perianal skin at the distal extent of the haemorrhoidal tissue.
- The haemorrhoid is then dissected from the underlying internal sphincter.
- As the pedicle of the haemorrhoid is reached, vessels are controlled by diathermy or an absorbable transixion stitch, taking cre not to include the internal sphincter.
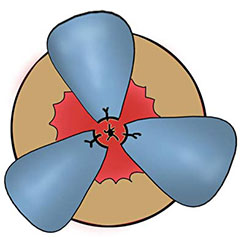
- The haemorrhoid is excised & the process is repeated for each haemorrhoid. Take care to leave skin & muscosal bridges between each resection to prevent anal stenosis.
- Some surgeons leave the wounds open & some close them with an absorbable suture.
Postoperative Management
- Encourage regular baths.
- Prescribe analgesics & a laxative to offset constipation.
- Continue oral metronidazole for five days.
Main Postoperative Complications
Pain, haemorrhage, constipation & urinary retention.