Coronary Artery Bypass
Preioerative Preparation
Includes careful general assessment & coronary angiography.
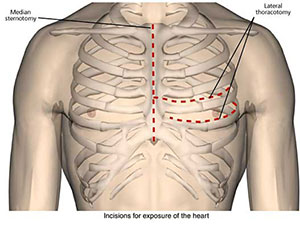
Incision
Median sternotomy. (see Respiratory Systems Resource Panel)
Procedure
- Prepare the internal mammary artery or harvest the long saphenous vein from one leg.
- Open the pericardium vertically.
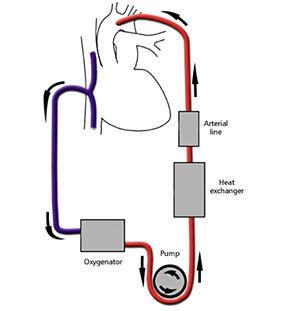
- Establish cardio pulmonary bypass.
- First, give heparin (3mg/kg).
- Place a purse-string suture in the ascending aorta.
- Pass an arterial catheter through the purse-string, secured to a tourniquet.
- Next, pass a large bore cannula (or cannulas to the SVG & IVC) for venous drainage through a purse-string in the right atrium & tie it to a tourniquet.
- Connect these to a perfusion circuit which includes a roller pump, an oxygenator, a heat exchanger, a cardiotomy suction & an arterial line filter.
- A cardioplegia solution (Hartmanns plus potassium at 4° introduced proximal to the corss-clamped aortic root produces asytolic arrest & prolongs ischaemic time.
- Next, identify the coronary artery to be bypassed.
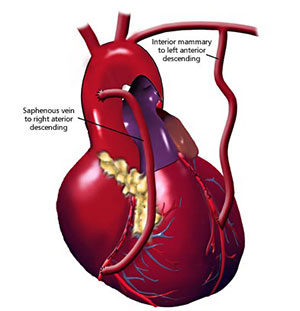
- If selected, a vein graft should be reversed. The proximal portion of the vein is anastomosed to the ascending aorta & its bevelled distal end is anastomosed to an arteriotomy in the coronary artery distal to the stenosis.
- The internal mammary artery is a preferable conduit due to its long-term patency. The distal end of the internal mammary may be anastomosed to the left anterior descending coronary artery while its proximal portion is left attached to the subclavian artery.
Closure & Drainage
The pericardium is closed over a suction drain & steel wires are used to close the sternum.
Main Postoperative Complications
Include complications of bypass, cardiac arrythmias, thrombo-embolism & bleeding.