Pilonidal Sinus Excision
Many procedures are described but none, judging by the length of healing & recurrence, is perfect. Procedures include curettage of the tract, phenol injection, marsupialisation, excision & primary closure, & asymmetric closure (Bascom or Karydakis). In addition, the complexity of the sinus & the presence of sepsis must be considered. Here we describe excision & primary closure.
Preoperative Preparation
- A pre-existing pilonidal abscess should be incised & drained.
- Consider prophylactic antibiotics, if primary closure is planned.
Anaesthesia
General or spinal anaesthesia
Position
Prone, with the buttocks taped apart to open the natal cleft, which is shaved.
Procedure
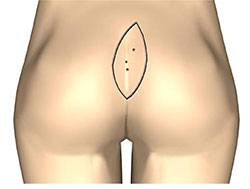
Define the anatomy of the sinus tract & any offshoot tracks from the main sinus:
- This may be achieved by inserting a fine probe into the sinus & laying it open while following the tract or its branches to their farthest extent. Alternatively, injection of methlene blue dye into the track may help identification & dissection.
- Any hairs, pus or debris are removed.
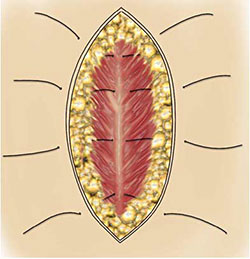
- The tract is then excised using careful haemostasis. The excision usually extends to the fascia overlying the sacrum.
Closure & Drains
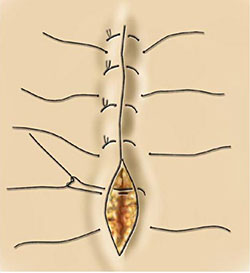
- In the absence of active infection the wound is closed primarily. This may be achieved by the insertion of 3-4 deep tension sutures, taking wide & deep bites to include the sacral fascia.They are left untied.
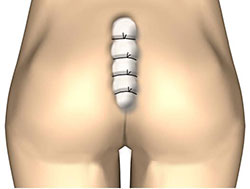
- Next, having released the buttocks, approximate the skin accurately with non-absorbable mattress sutures.
- Finally, tie the tension sutures snugly, but not tightly, over a rolled gauze swab to achieve deep haemostasis.
- Some surgeons use a closed suction drain.
Postoperative Management
The tension sutures are removed at one week and sutures at 10-14 days.
Main Postoperative Complications
Infection, wound breakdown & recurrence.