Left Hemicolectomy/Sigmoid Colectomy
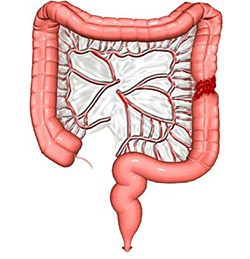
- After a full laparotomy, mobilise the left colon & sigmoid by dividing the 'congenital' adhesions & the peritoneal reflection to the posterior abdominal wall. Care is taken to identify & preserve the ureter & gonadal vessels.
- The mobilisation usually extends from below to up around the splenic flexure along the gastrocolic ligament. The greater omentum is freed off the transverse colon, to the left side of the middle colic artery arcade, after gaining a window into the lesser sac. Care is teken not to tear the spleen during this dissection.
- Open a mesocolic windows between the vessels with diathermy.
- The left colic & inferior mesenteric arteries are identified, divided & suture ligated. During left colon cancer surgery it is important to ligate the inferior mesenteric vein before mobilising the tumour to prevent tumour emboli. Also, a flush ligation of the inferior mesenteric artery is aimed at retrieving all draining lympgh nodes.
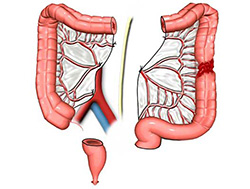
- Divide the left transverse & distal sigmoid colon using a linear cutting stapler.
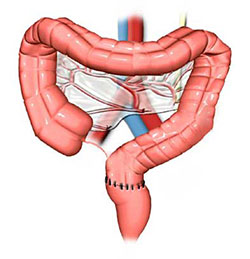
- The two ends of bowel are then brought together to construct a colo-colic anastomosis. The mesocolic defect is closed.