Hepatic Resection
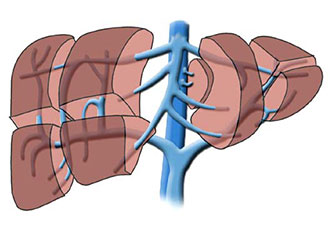
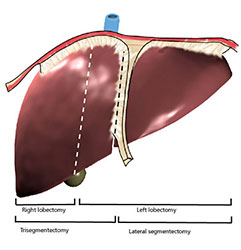
Most resections are carried out for tumours. The techniques of hepatic lobectomy, trisegmentectomy, segmentectomy & even non-anatomical resections have been developed based on our knowledge of the anatomy of the liver & its blood supply to the various lobes & segments. A detailed description of all the various resections is beyond the cope of this text but the principles of resection, beyond that required for a simple wedge excision will be outlined.
Preoperative Preparation
- Includes detailed imaging of the liver & tumour anatomy as well as a metastic work-up.
- Laparoscopic evaluation of the peritoneal cavity may be considered.
Procedure
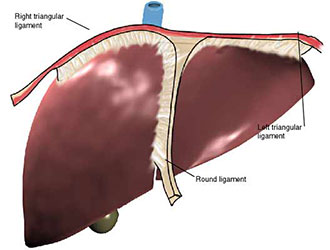
The liver should first be fully mobilised by dividing the left triangular ligament to the oesophageal hiatus, the round ligament, & the right triangular ligament back to the bare area.
- The liver can now be assessed by intra-operative ultrasound to gauge the extent of resection required.
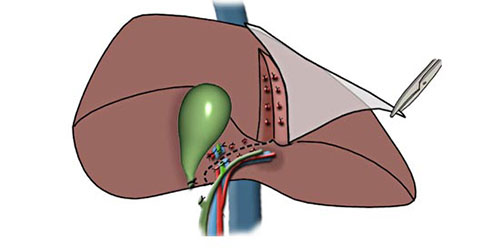
- The liver vascular inflow & outflow should be controlled before parenchymal division.
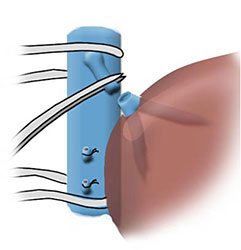
- The Pringle manouevre controls the entire hepatic inflow but may result in hepatic ischaemia & re-perfusion injury after unclamping. It is better to achieve one-sided vascular control of the hepatic arterial & portal flow to the liver.
- To display these vessels it is first necessary to dissect & separate them & the common bile duct with slings in the hepatoduodenal ligament.
- The vascular outflow of the liver may be controlled by dissection of the hepatic beins at the vena cava. Resection can now proceed.
- The selected vascular inflow & outflow are clamped & the liver is seen to demarcate.
- Parenchymal division proceeds along the line of demarcation & is facilitated by the use of the 'finger' fracture technique or an argon beam or ultrasonic dissector.
- Exposed vessels & ducts along the line division are clipped, sutured, sealed or stapled.
After the specimen is delivered the raw surface of the liver may be sealed with argon plasma coagulation.
Closure & Drainage
Routine closure with ample drainage from the raw liver surface.
Main Postoperative Complications
Include prolonged drainage of bile.